
Neurologic PET
Exploring neurological indications in PET and PET/CT
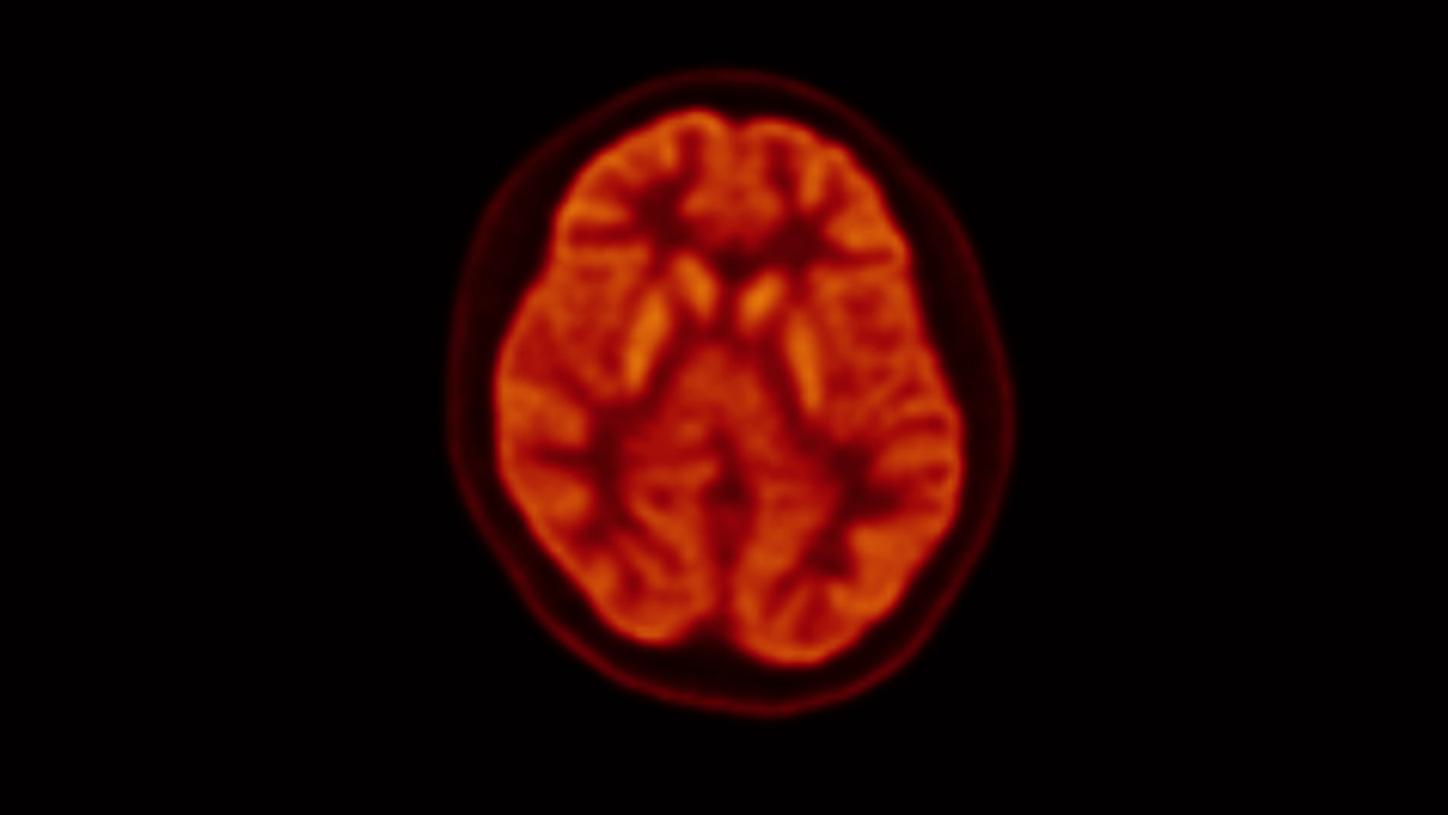
PET brain imaging provides a functional assessment and observes brain activity and metabolic processes. PET effectively detects beta-amyloid plaque, tau deposits, glucose or amino acid metabolism, and dopamine receptors in the brain.1 PET brain imaging can often detect changes in brain function and metabolism before other conventional imaging modalities like MRI or CT scans. Early detection can be vital for diagnosing neurological conditions sooner when interventions may be more effective. Alzheimer's Disease, Parkinson's Disease, and Epilepsy are common indications for PET neuroimaging.
Alzheimer's Disease
An early diagnosis can offer the patient and their family valuable time to make decisions regarding medical care and needs.
The value of knowing


For loved ones
- Participate in planning of care for their loved one
- Address safety issues and concerns

β-amyloid imaging
"SNMMI applauds CMS for recognizing the pivotal role of amyloid PET scans in effectively managing Alzheimer's and other dementias"11

Healthy brain
β-amyloid protein fragments are broken down and removed from the brain

Alzheimer's disease brain
β-amyloid protein fragments accumulate to form hard, insoluble plaques between neurons
Data has shown that beta-amyloid plaques can begin to accumulate 20-25 years before the clinical onset of the disease, suggesting that β-amyloid is involved in the pathophysiology of AD.7 The use of β-amyloid PET imaging may help enable the quantification of β-amyloid plaque burden in the brain cortices as well in the blood vessels supplying the brain. Because β-amyloid plaques are found in all patients with AD, the use of β-amyloid PET imaging may play an important role in diagnosis.12 A positive β-amyloid PET scan is not a definitive diagnosis for Alzheimer's disease but rather a diagnostic tool to determine the presence of β-amyloid plaques in the brain to help increase the clinical certainty of AD diagnosis.12
β-amyloid plaques

Data courtesy of University TN Medical Center, Knoxville, TN, USA
β-amyloid plaques are seen in other neurologic conditions and older people with normal cognition; therefore the confirmation of β-amyloid plaques does not definitively lead to AD diagnosis.

Access to beta-amyloid
PETNET produces and delivers beta-amyloid and tau PET imaging biomarkers for Alzheimer's disease and other neurological PET studies across the United States. The SNMMI offers a map locator to find hospitals or imaging centers offering beta-amyloid PET. SNMMI Brain imaging portal
Theranostics for neurodegenerative diseases
In April of 2022, CMS announced that all USFDA-approved anti-amyloid immunotherapies would be subject to coverage with evidence development (CED) for patients with a clinical diagnosis of mild cognitive impairment (MCI) due to AD or mild AD dementia, both with confirmed presence of β-amyloid buildup consistent with AD.14 The October 13, 2023 decision by CMS to eliminate the CED requirements and allow MACs to determine appropriate coverage will lead to improved accessibility to beta-amyloid imaging and evaluate the use of new therapies as they become available.
Research and drug development are dynamic, with new drugs and therapies often emerging; as of January 2024, there are currently two FDA-approved drugs to treat patients with early-stage Alzheimer's disease.

Parkinsonian syndromes
Refractory seizures
Types of epilepsy
18F FDG PET/CT imaging is indicated for assessing patients with refractory epilepsy for pre-surgical evaluation.19 Epilepsy is a neurological disorder characterized by epileptic seizures caused by excessive neuronal activity in the brain. This neurological disorder affects approximately 65 million of the world’s population, with approximately 20%-40% of those diagnosed with refractory epilepsy.20 There are four main types of epilepsy:
Fludeoxyglucose F 18 Injection (18F FDG)
Sharp cortical and striatal definition in pediatric patient with epilepsy

Coronal

Sagittal
Small structures like superior colliculi and cerebellar peduncles sharply visualized due to high resolution
Axial
No clear foci of interictal hypometabolism suggestive of epileptic foci delineated
Identifying the ictal onset zone may provide improved management and surgical outcomes. Non-invasive techniques like EEG monitoring, magnetic resonance imaging (MRI), single photon emission tomography/computed tomography (SPECT/CT), and 18F FDG PET may be helpful in the localization of the seizure focus.20
18F FDG measures glucose metabolism related to the synaptic and neuronal activity of the brain tissue.23 Most often, 18F FDG PET imaging is performed during the interictal phase as the ictal phase is unpredictable and makes imaging difficult due to the necessary resources required for the exam. Postictal imaging can be challenging to interpret, and uptake can vary depending on the timing of the 18F FDG injection.20 The uptake pattern with interictal 18F FDG PET may be affected by recent or ongoing seizure activity; thus, the use of electroencephalography (EEG) recording before and during the scan will assist in identifying when a seizure may be occurring.20
Many studies have shown that 18F FDG PET may help predict surgical outcomes for patients with refractory epilepsy. In addition, 18F FDG has shown superior sensitivity for those with an equivocal MRI and EEG in determining the pre-surgical localization of epileptogenic foci with those with medically refractory partial epilepsy.20
18F FDG PET imaging is CMS-approved in the US for pre-surgical evaluation for the purpose of localization of a focus of refractory seizure activity.24
Important safety information
Fludeoxyglucose F 18
Fludeoxyglucose F 18
Indications & usage
Fludeoxyglucose F 18 Injection (18F FDG) is indicated for positron emission tomography (PET) imaging in the following settings:
- Oncology: For assessment of abnormal glucose metabolism to assist in the evaluation of malignancy in patients with known or suspected abnormalities found by other testing modalities, or in patients with an existing diagnosis of cancer.
- Cardiology: For the identification of left ventricular myocardium with residual glucose metabolism and reversible loss of systolic function in patients with coronary artery disease and left ventricular dysfunction, when used together with myocardial perfusion imaging.
- Neurology: For the identification of regions of abnormal glucose metabolism associated with foci of epileptic seizures.
Important safety information
- Radiation Risk: Radiation-emitting products, including Fludeoxyglucose F18 Injection, may increase the risk for cancer, especially in pediatric patients. Use the smallest dose necessary for imaging and ensure safe handling to protect the patient and health care worker.
- Blood Glucose Abnormalities: In the oncology and neurology setting, suboptimal imaging may occur in patients with inadequately regulated blood glucose levels. In these patients, consider medical therapy and laboratory testing to ensure at least two days of normoglycemia prior to Fludeoxyglucose F 18 Injection administration.
- Adverse Reactions: Hypersensitivity reactions with pruritus, edema, and rash have been reported. Have emergency resuscitation equipment and personnel immediately available.
Dosage forms and strengths
Multiple-dose 30 mL and 50 mL glass vial containing 0.74 to 7.40 GBq/mL (20 to 200 mCi/mL) Fludeoxyglucose F 18 Injection and 4.5 mg of sodium chloride with 0.1 to 0.5% w/w ethanol as a stabilizer (approximately 15 to 50 mL volume) for intravenous administration.
Fludeoxyglucose F 18 Injection is manufactured and distributed by:
PETNET Solutions, Inc.
810 Innovation Drive
Knoxville, TN 39732
These highlights do not include all the information needed to use Fludeoxyglucose F 18 Injection safely and effectively.
Download full prescribing info
Did this information help you?
All rights reserved. All product/company names mentioned herein are the trademarks of their respective owners
Lattanzi S, Brigo F, Vernieri F, Silvestrini M. Visit-to-visit variability in blood pressure and Alzheimer's disease. J Clin Hypertens (Greenwich). 2018 May;20(5):918-924. doi: 10.1111/jch.13290. Epub 2018 Apr 25. PMID: 29693801; PMCID: PMC8031352.
Alzheimer’s Association, 2021 Alzheimer’s Disease Facts and Figures, Alzheimer’s Dement 2021; 17(3)
Mayo Clinic Staff. “Alzheimer's Stages: How the Disease Progresses.” Mayo Clinic, Mayo Foundation for Medical Education and Research, 29 Apr. 2021, https://www.mayoclinic.org/diseases-conditions/alzheimers-disease/in-depth/alzheimers-stages/art-20048448.
Mayo Clinic Staff. “Learn How Alzheimer's Is Diagnosed.” Mayo Clinic, Mayo Foundation for Medical Education and Research, 7 May 2022, https://www.mayoclinic.org/diseases-conditions/alzheimers-disease/in-depth/alzheimers/art-20048075.
Bateman, Randall J., et al. "Clinical and biomarker changes in dominantly inherited Alzheimer's disease." N Engl J Med 367 (2012): 795-804.
Alzheimer’s Association. (2021). Alzheimer’s disease facts and figures. [Ebook]. Chicago. Retrieved from https://alz.org/media/Documents/alzheimers-facts-and-figures-2021.pdf
“Alzheimer's Disease Fact Sheet.” National Institute on Aging, U.S. Department of Health and Human Services, https://www.nia.nih.gov/health/alzheimers-disease-fact-sheet.
Lattanzi S, Brigo F, Vernieri F, Silvestrini M. Visit-to-visit variability in blood pressure and Alzheimer's disease. J Clin Hypertens (Greenwich). 2018 May;20(5):918-924. doi: 10.1111/jch.13290. Epub 2018 Apr 25. PMID: 29693801; PMCID: PMC8031352.
Chen B, Marquez-Nostra B, Belitzky E, et al. PET Imaging in Animal Models of Alzheimer's Disease. Front Neurosci. 2022;16:872509. Published 2022 May 24. doi:10.3389/fnins.2022.872509
FOR HEALTHCARE PROFESSIONALS Frequently asked questions about beta-amyloid imaging. (2021) https://www.alz.org/media/documents/health-care-pros-faqs-beta-amyloid-imaging.pdf
“About Us New IDEAS Study.” About Us, https://www.ideas-study.org/About-Us#:~:text=The%20New%20IDEAS%20study%20will%20also%20have%20two%20additional%20objectives,have%20consented%20to%20blood%20collection.
“Monoclonal Antibodies Directed against Amyloid for the Treatment of Alzheimer's Disease.” CMS.gov Centers for Medicare & Medicaid Services, https://www.cms.gov/medicare-coverage-database/view/ncacal-decision-memo.aspx?proposed=Y&NCAId=305.
Kumar A, Chugani HT. The role of radionuclide imaging in epilepsy, Part 1: Sporadic temporal and extratemporal lobe epilepsy. J Nucl Med. 2013;54(10):1775-1781. doi:10.2967/jnumed.112.114397
Hodolic M, Topakian R, Pichler R. (18)F-fluorodeoxyglucose and (18)F-flumazenil positron emission tomography in patients with refractory epilepsy. Radiol Oncol. 2016;50(3):247-253. Published 2016 Jul 19. doi:10.1515/raon-2016-0032
“4 Types of Epilepsy, Their Symptoms, and Treatments.” Medical News Today, MediLexicon International, https://www.medicalnewstoday.com/articles/types-of-epilepsy#contacting-a-doctor.
Sarikaya I. PET studies in epilepsy. Am J Nucl Med Mol Imaging. 2015;5(5):416-430. Published 2015 Oct 12
Fisher, Dr. Robert S, et al. “Operational Claissification of Seizure Types by the International League Against Epilepsy’ Position Paper of the ILAE Commission for Classification and Terminology.” Https://Onlinelibrary.wiley.com/Doi/Epdf/10.1111/Epi.13670, Wiley Online Library, 8 Mar. 2017, https://onlinelibrary.wiley.com/doi/epdf/10.1111/epi.13670.
Stanescu, Luana, et al. “FDG Pet of the Brain in Pediatric Patients: Imaging Spectrum with MR Imaging Correlation.” RadioGraphics, 30 Aug. 2013, https://pubs.rsna.org/doi/10.1148/rg.335125152.
CMS.GOV. “FDG Pet for Refractory Seizures.” CMS.gov Centers for Medicare & Medicaid Services, https://www.cms.gov/medicare-coverage-database/view/ncd.aspx?NCDId=294&NCDver=1.